40 yr female with burning sensation of palms
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
Case
A 40 yr old female pt with
chief complaints of burning sensation in palms since 2 months insidious in onset , gradually progressive increased intensity at night is seen
Not associated with tingling sensation , numbness,paresthesias .
No c/o polyphagia,polydypsia,polyuria,nocturia
K/c/o diabetes mellitus since 3 yrs
On medication glimi M1 po od
Past history
She has no similar complaints in past.
Is not a known case of htn,tb,asthma,seizures, thyroid disorders.
Pt got diagnosed as diabetic when visited a hospital for regular checkup 3 yrs ago
She is uneducated and working as a laundry iron woman since childhood (from 15 yrs) she got married in teenage (at 15 yrs) .Has her first child ( at 16yrs) and second child at 18 yrs . Both the babies delivered through LSCS due to baby wt (4 kg) .
Diet : mixed
Appetite : normal
Bowel and bladder : regular
Sleep : inadequate due to complaints
Addiction: none
General examination
Patient is conscious , coherent, co operative
No
Icterus
Cyanosis
Clubbing
Lymphadenopathy
Oedema
Pallor : present





Temp:98.5°F
Bp: 140/80 mmhg
PR:84 bpm
RR: 18cpm
Systemic examination
Cvs :
Precordium normal
No thrills ,
On auscultation
S1,S2 heard ,no murmurs
CNS:
Higher mental functions :intact
Cranial nerves :intact
Motor system:Normal power,tone,Gait
Reflexes:normal
Sensory examination:Normal
No meningeal signs
Tremors : absent
Rs:
Shape of chest:Bilaterally symmetrical, Elliptical in shape
No visible chest deformities
No kyphoscoliosis,
Abdomino thoracic respiration, No irregular respiration
Trachea is central
Auscultation:
Normal vesicular breath sounds heard
P/A
INSPECTION:
Shape of abdomen:Distended
Umbilicus:inverted
Skin over the abdomen is normal with striae.
All quadrants are moving equally with respiration
No visible peristalsis, Hernial orifices intact
External genitalia normal
PALPATION:
Temperature:Not raised
Tenderness:Absent
No Rebound tenderness
No guarding rigidity
No organomegaly
Percussion
No shifting dullness ,
No fluid thrill
Auscultation
Bowel sounds are heard.
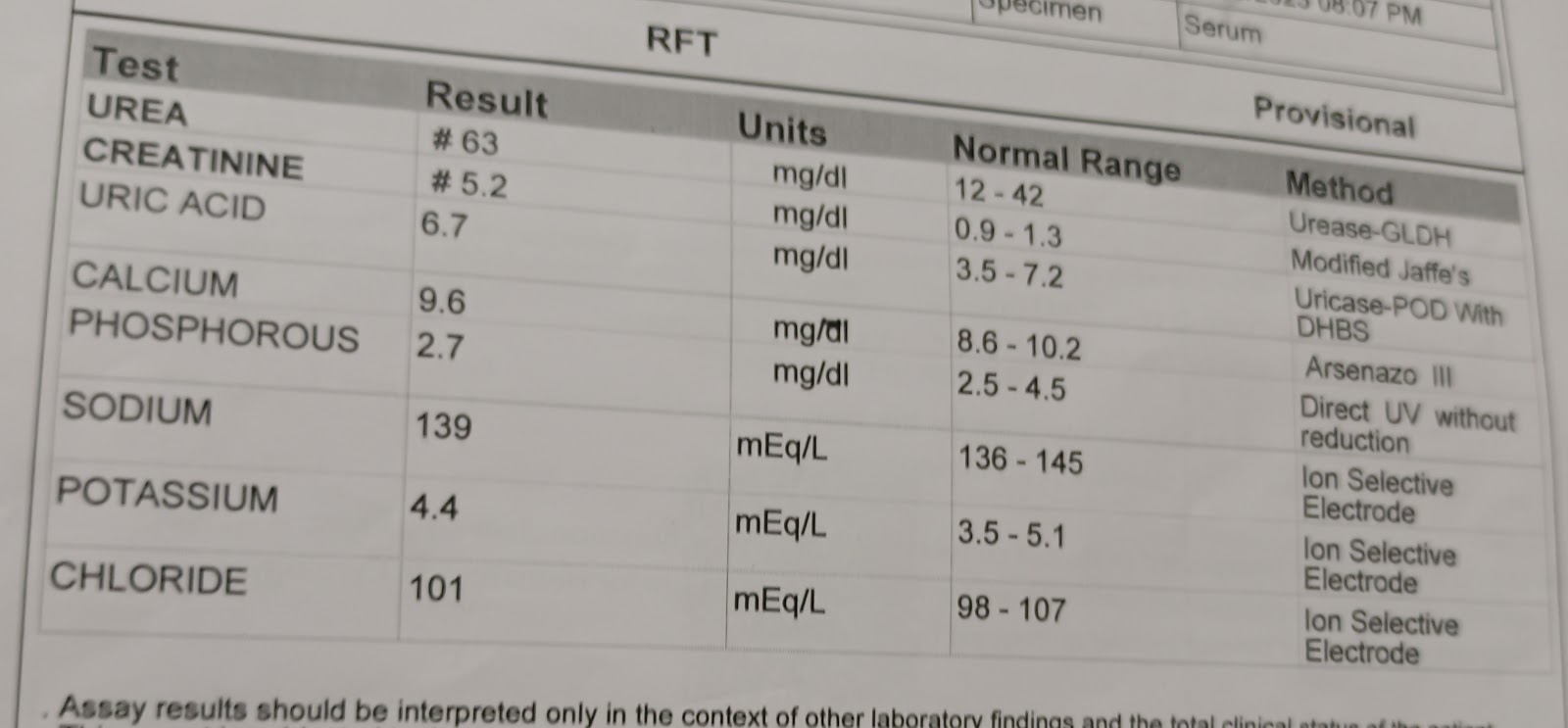
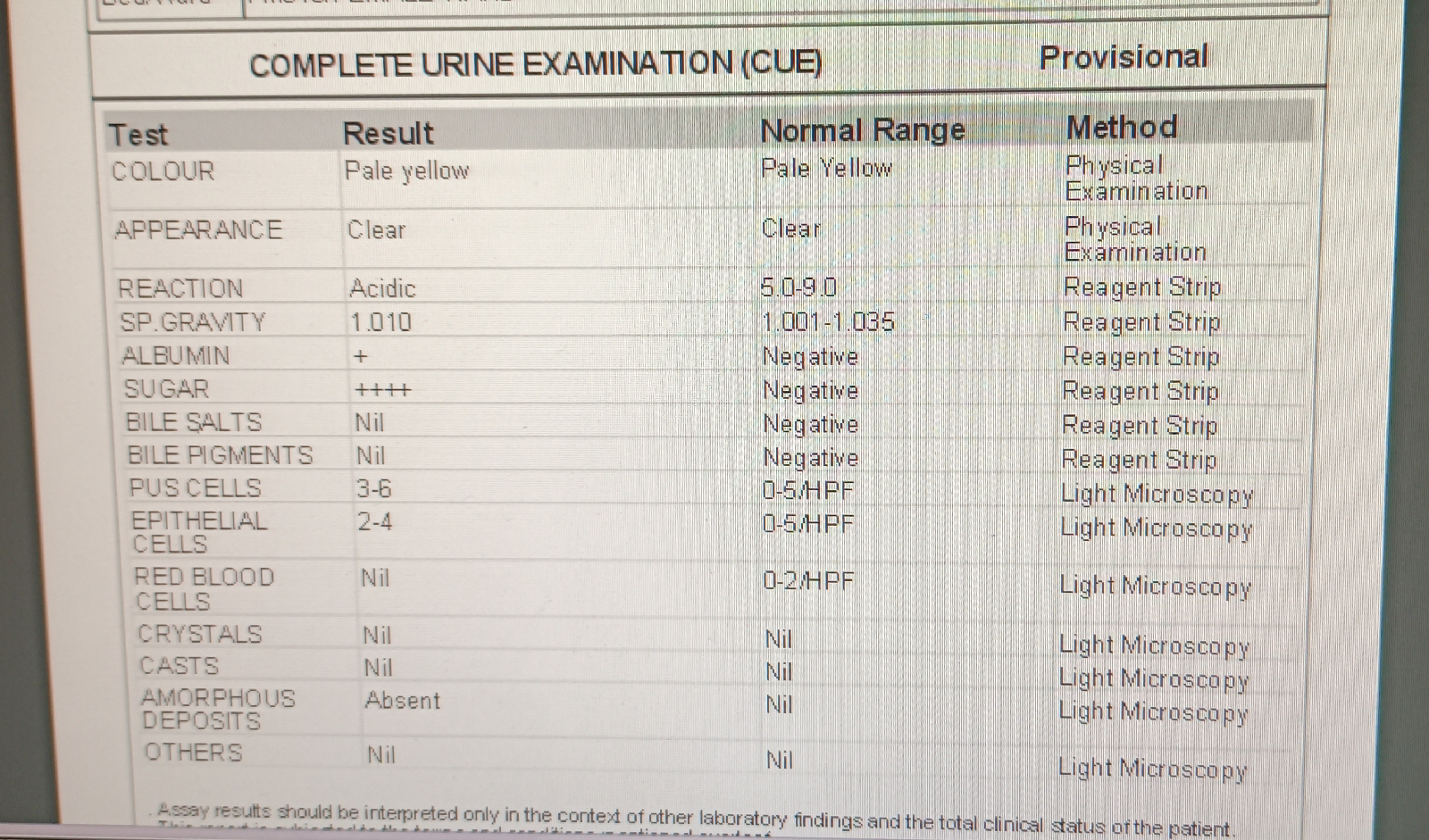
Investigations
On 3/7/23

FBS : 246 MG/DL
PLBS: 410 MG/ DL
HbA1C: 7.4%
Serum creatinine :0.6 mg/DL
ECG:

On 4/7/23


Blood urea : 24 mg/dl
Serum creatinine : 0.7 mg/dl
Stool for occult blood : negative
Reticulocyte count : 1%
Serum ferritin : 3.1 ng/ml
Normal 11- 306.8
Serum iron : 42 ug/dl
Chest x ray PA view

On 4/7
5 pm: 254
7pm.: 248
10 pm :312 inj . hai 4 nph 6
On 5/7
2am: 243
8 am: 245 inj hai nph 6 units each
10 am : 98
1pm 305 10units hai
On 4/7
5 pm 254
7pm. 248
10 pm 312 hai 4 nph 6
On 5/7
2am 243
8 am 245 hai nph 6 units each
10 am 98
1pm :305 10units hai inj
4 pm :331
7 pm ;211 inj 6 units each hai,nph
10 pm : 201
On 6/7
2 am :172
8 am :253
4 pm: 331
7 pm: 211 6 units each hai,nph inj
10 pm: 201
On 6/7
2 am :172
8 am: 253
Diagnosis
Uncontrolled sugars
K/c/o DM 2 since 3 yrs
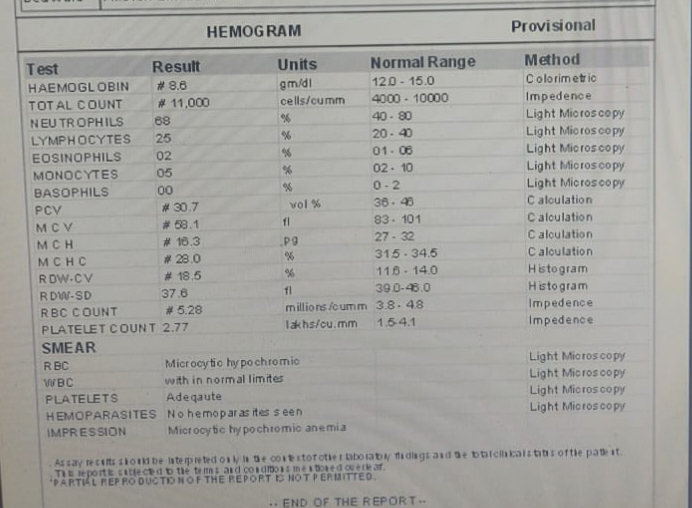
Iron deficiency anemia secondary to nutritional /blood loss
Treatment
Inj HAI s/c tid acc to grbs
8 am ,2 pm,8 pm
Inj nph sc/bd
Inj iron sucrose 200 mg in 100 ml ns /iv /bd
Tab orofer xt po/od
Tab limcee po/od
Patient got discharged on 7/7
Advised
Inj hai 10 units sc/tid
Inj nph sc /bd 8 units
8 am,8 pm
Tab .orofer. Xt po/od for 1 month
Tab . Limcee po/od for 1 week