70 yr old male patient with shortness of breath ,pedal oedema
70 year old male patient presented to the casuality with the
CHIEF COMPLAINTS:-
S.O.B since 15 days
loss of appetite since 15 days
decreased urine output since 10 days
pedal oedma since 10 days
HISTORY OF PRESENTING ILLNESS:-
He was apparently asymptomatic 14 years back then he suddenly developed slurred speech and was observed having an abnormal gait.
then he was taken to a neuro surgeon where he was managed conservatively for a week and was on medication for 4 years . ( medication unknown, indication unknown).
Then after 4 years he was having severe SOB and was taken to a hospital where he was diagnosed with COPD and the medication dose was decreased and his symptoms subsided.
In 2018 , then he had a traumatic injury to the leg which was not healing and was taken to thehospital where rountine check up was done to find to have Type 2 DM .
Then in 2021 he developed bilateral pedal edema and on investigations it was found that CREATININE was high and diagnosed as CKD
and Now he presented with the SOB since 10-15 days. Grade 4 since 3 days.i.e.,( SOB on rest
not associated with palpitations, sweating
loss of appetite since 15 day
decreased urinary output since 10 days
No history of hematuria, burning micturition.
Bilateral pitting type of pedal edema since 10 days
he was taken to a local hospital where they found to have higher creatinine and was sent here for further management.
PAST HISTORY:-
HTN since 14 years and on medication since then
( drug dose unknown)
DM since 4 years and on medication ( drug and dose unknown
known case of CKD since 2 years
no history of TB ,Asthma ,CAD,leprosy.
PERSONAL HISTORY:-
Diet - mixed
appetite - decreased
bowel and bladder - Regular
sleep - adequate
Addictions - smoked for 15 years and stopped smoking after diagnosed with COPD in 2012 .
occasionally alcohol
No surgeries done in the past.
FAMILY HISTORY:-
No relevant family history
ALLERGIC HISTORY:-
no allergies for any kind of drugs and food.
GENERAL EXAMINATION:-
patient was semi - conscious and is on ventilator
not well nourished and weakly built.
Pallor present.
No icterus
No cyanosis
No clubbing
No lymphadenopathy
pitting type of edema (bilateral)
VITALS:-
Temperature:- febrile
P.R :- 100
R.R :- 24
BP :- not measured
GRBS :- 177mg%


SYSTEMIC EXAMINATION:-
RESPIRATORY SYSTEM:-
INSPECTION:-
Antero - posterior diameter increased
on inspection and palpation:- Trachea is central
AUSCULTATION:-
Bilateral air entry present .
FINE CREPTS are heard on 4 areas
right and left infra axillary
and right and left infra scapular .
CARDIO VASCULAR SYSTEM:-
S1 ,S2 heard
No Murmurs heard
PER ABDOMEN
shape of abdomen:- Scaphoid
no temderness
no palpable organs
bowel sounds - present
CENTRAL NERVOUS SYSTEM:-
patient is semi conscious .
Signs of meningeal irritation:- negative
cranial nerves - not done as he is on ventilation
sensory system - not done
motor system - not done
INVESTIGATIONS:-
Random blood sugar on 31/7/22 :-

LFT on 31/7/22 :-

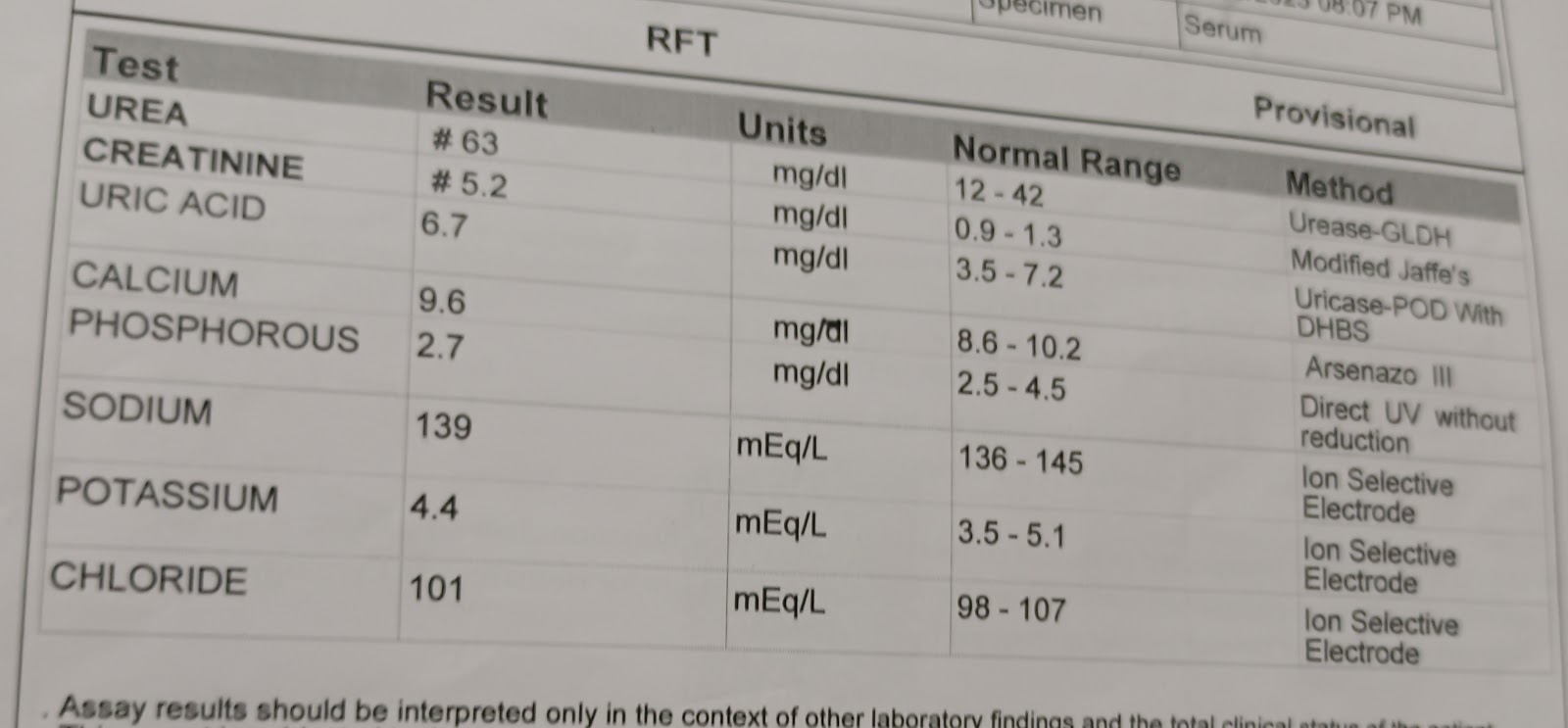
RFT on 31/7/22 :-

Serum Iron on 31/7/22 :-

HEMOGRAM On 31/7/22:-

BLOOD GROUPING :- A Group( +ve )
SEROLOGY:- Anti HCV ab -non reactive
HIV RAPID TEST -NON REACTIVE
HBs Ag rapid - negative
ABG on 31/7/22:-

X ray on 31/7/22 at 10:46 am

ABG on 1/8/22:-

ECG on 1/8/22 :-

RFT on 1/8/22 :-

LFT on 1/8/22 :-

X ray on 1/8/22 on 3:06 am

X ray on 1/8/22 on 12:25 pm

ABG on 2/8/22:-

X ray on 2/8/22 at 7:11 am

ABG on 3/8/22 :- at 8:00 am

Blood urea on 3/8/22:-

Haemogram on 3/8/22:-

Serum creatinine on 3/8/22:-

Serum electrolytes on 3/8/22:-

ABG at 3:00 am :-

ABG at 5:30 pm :-

ABG at 4/8/22:-6:00am

RFT on 4/8/22:-

DIAGNOSIS:-
Acute excerbation of COPD.
CKD secondary to diabetic nephropathy
Anemia of chronic disease.
HTN since 14 years, Type 2 DM since 4 years.
PLAN OF CARE :- Supportive management
TREATMENT:-
1) Fluid restriction less than 2L/day
2)Salt restriction
3) NEB - DUOLIN 8 th hrly
BUDECOID 12 hrly
4) I.V PIPTAZ 2.25 gm IV BD
5) I.V PAN 40 mg BD
6)LASIX 60 mg IV BD
7) HYDRO CORTI 100 mg
8) INJ NEOMOL 1g IV
9)INJ LEVOFLOX
10)INJ ERYTHROPOIETIN 4000 IU
11) T Shelcal 500 mg
12)NODOSIS 500 mg
13) GRBS charting 6 th hrly
14) vitls charting 4 th hrly
DEATH CERTIFICATE:-