53 yr old female with pedal oedema and shortness of breath
This is an online E log to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here, we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
53 yr old female patient came to opd with Chief complaints of
- Shortness of breath since 3 days ,pedal oedema since 4 days.
History of presenting illness:
Patient was apparently asymptomatic , noticeable events as -12 yr back she had high grade fever then she visited govt hospital,she was treated and then 4yr back she was diagnosed with hypertension on symptoms of chronic neck pain ,giddiness , headache and medicated to it.
10 months back she developed shortness of breath ,she visited the hospital ,investigations revealed blood urea and creatinine levels being raised .
She was diagnosed with renal failure ,undergoing dialysis weekly twice along blood transfusion
She has noticeable shortness of breath ,pedal oedema 4 days back.
Her pedal oedema is resolved .
Past history:
History of hypertension since 4 yrs.
NO H/O DM, ASTHMA , TB, EPILEPSY.
Personal history:
Appetite - normal
Diet - mixed
Bowel movements - regular
Bladder - Decrease urinary output
No addiction
Family history:
No significant family history
General examination:-
Patient was consious,coherent,and cooperative,well oriented with time ,plac e,person.
Pallor - present
Icterus - absent
Clubbing - absent
Cyanosis - absent
Lymphadenopathy - absent
Oedema - bilateral pedal oedema which is pitting type and grade 2
Oedema subsided later.



Temperature 98.7°F
Blood pressure: 140/90
Respiratory rate :20
Pulse rate :90
Sp02:98%
Systemic examination;
CVS
Normal s1 and s2 sounds heard
No cardiac murmurs
RESPIRATORY SYSTEM
Normal vesicular breath sounds heard
Respiratory crepts present on right
P/A
Soft, non tender, bowel sounds- normal
CNS
no focal neural defecits, GCS - 15/15, no signs meningeal irritation, motor system normal.
Investigations
Hemogram
On 30/1




LFT

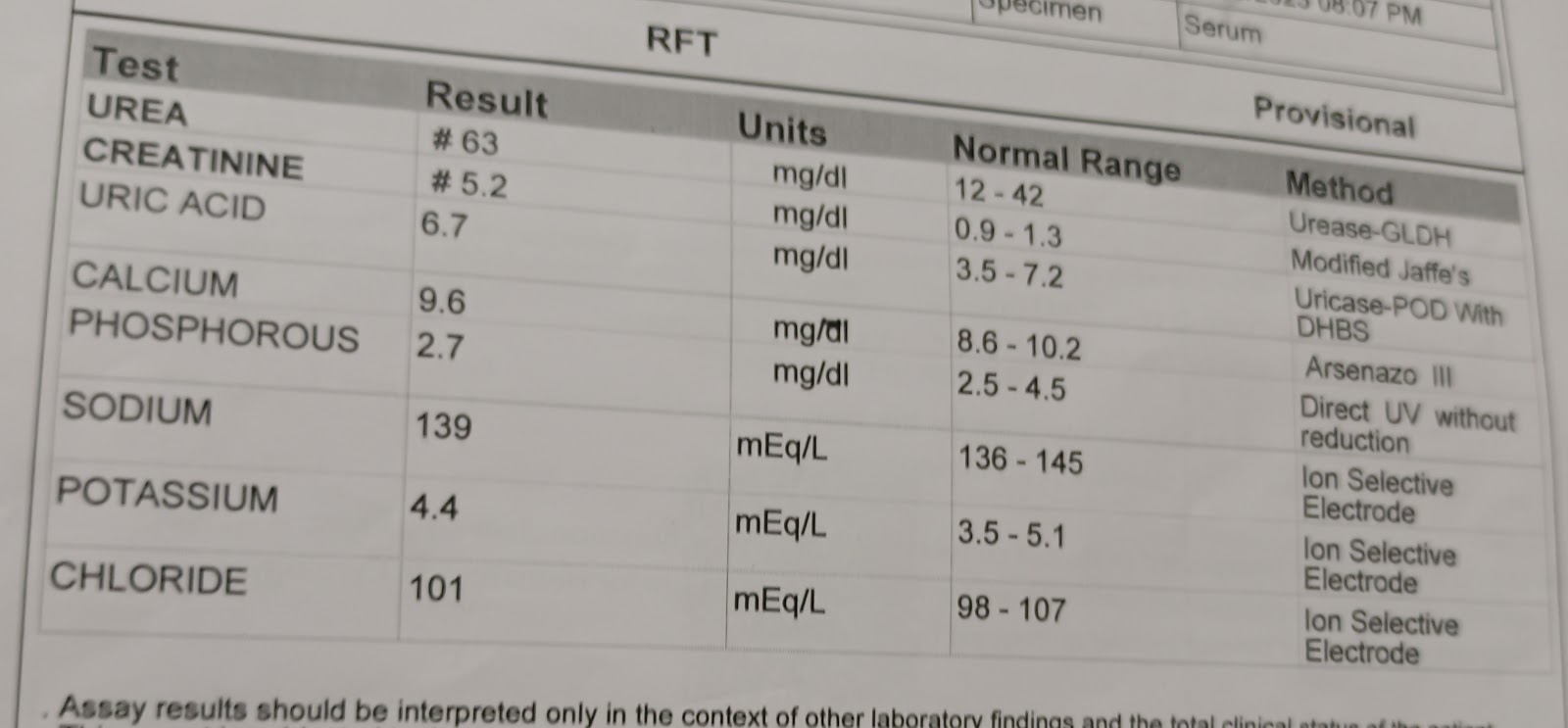
RFT


2D echo findings
Dilated RA,RV ,LA,concentric LVH +
Anterior wall hypokinetic,RWMA +
Ultra sound findings:
Moderate pleural effusion with collapsed underlying lung segment.{right}
Mild pleural effusion {left}
Mild pericardial effusion
Bilateral renal pelvic dilatation.
Provisional diagnosis
Chronic kidney disease on Maintenance hemodialysis.
Treatment:
On 31 /1
Tab lasix 40mg TID
Tab nicardia 10mg TID
Tab arkamine 0.1mg QID
Tab met-xl 50mg BD
Tab nodosis 500mg BD
On 1/2/22
Tab lasix 40mg TID
Tab nicardia 10mg TID
Tab arkamine 0.1mg QID
Tab met-xl 50mg BD
Tab nodosis 500mg BD
Tab order xl 0d
Tab shelcal 500mg OD
On 2/2
Tab lasix 40mg TID
Tab nicardia 10mg TID
Tab arkamine 0.1mg QID
Tab met-xl 50mg BD
Tab nodosis 500mg BD
Tab order xl 0d
Tab shelcal 500mg OD
Patient is advised on dialysis weekly twice.