A 50 yr old female with pedal edema,breathlessness and decreased urine output.
This is an online E log to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here, we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.







Case:
A 50 year-old woman came to the hospital with complaints of :
 pedal oedema , pitting of oedema
pedal oedema , pitting of oedema


Pedal edema since 6 months.
Shortness of breath which is since 2 months.
Decreased urine output since 1.5 months.
History of present illness :
The patient was apparently asymptomatic 6 months ago then has swelling in both her legs which was gradually progressive, extending to her knees, facial puffiness which was on and off for 6 months.
H/o increased shortness of breath since 2 months which aggravated to Grade 4 SOB since 10-15 days, a/w orthopnea, decreased sleep and appetite and nocturnal cough.
H/o decreased urine output since 1.5 months.
H/o excessive sweating, nausea and vomiting on and off since 2 months.
Past history :
She was diagnosed with DM, HTN 10 years ago for which she is on TAB. LINAGLIPTIN 5mg OD and TAB. CINOD 10mg OD.
No history of TB, Asthma , Epilepsy, CVD.
Personal history :
Diet- mixed
Appetite -decreased
Sleep -decreased
Bowel movements - regular
Family history :
Not significant
GENERAL EXAMINATION:
Patient is conscious , coherent and co operative
Pallor is present
No icterus,clubbing,cyanosis,
lymphadenopathy.
Bilateral pedal edema is seen,pitting type.
Clinical images :
Pallor - present
pedal oedema , pitting of oedema
Vitals:
Temp: 97.3 F
Bp: 140/90 mm Hg
Pulse rate: 87 bpm
Respiratory rate : 21 cpm
Grbs: 103 mg/dl
Spo2: 98%
Systematic examination:
CVS: S1 and S2 heard
RS: BAE +, diffuse inspiratory crepts +
P/A: soft , non tender
CNS: no focal neurological deficits.
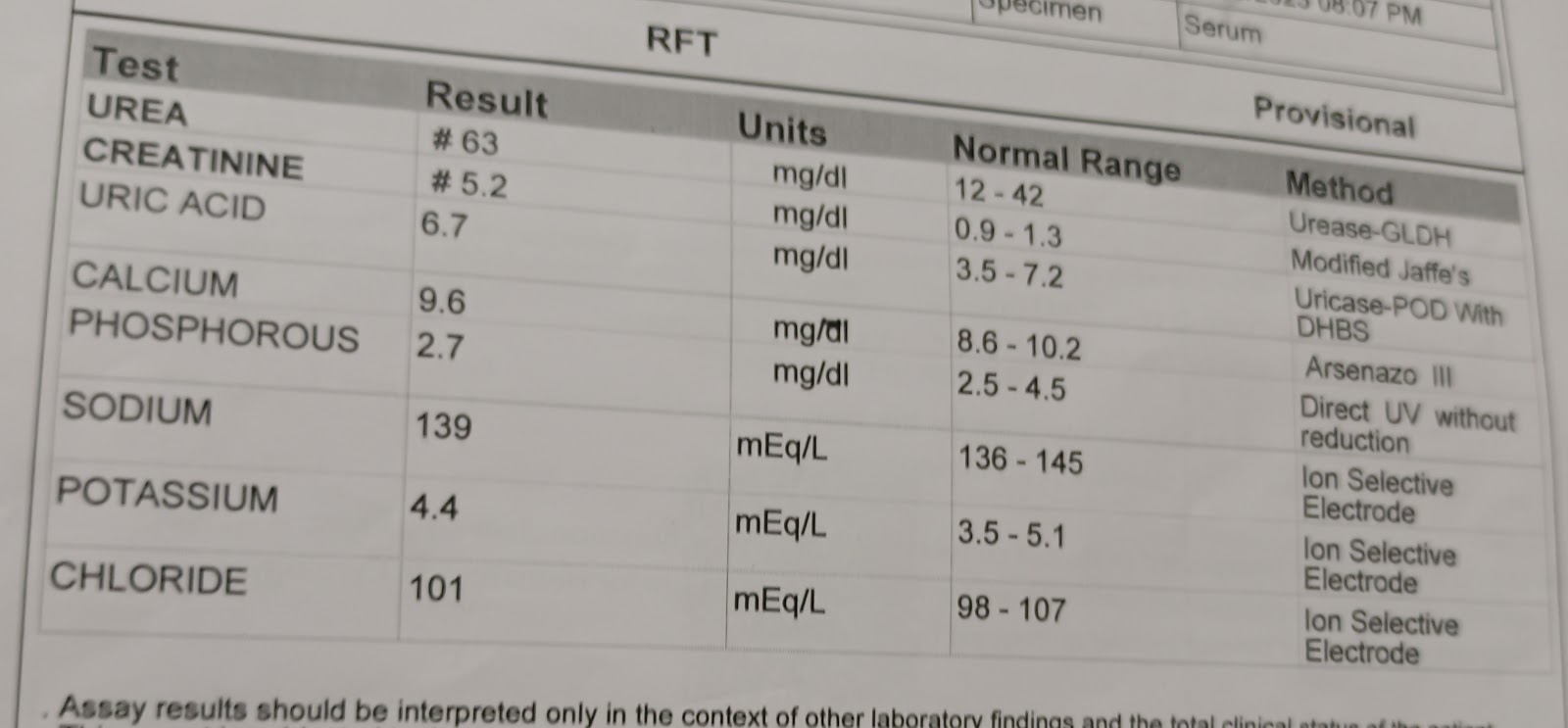
Investigations:
Hemogram :
Hb : 8.4 gm/dl
TLC : 6,100 cells/cu mm
Platelet count : 3.34 lakh/ cu mm
PCV : 25.5%
RBC count : 2.66 million/ cu mm
Blood group: O +
2 D echo : RA, RV, LA, LV Dilated, EF 30%.
Impression - Moderate to severe MR, Moderate TR with PAH, Mild AR. RWMA, LCX Akinetic, LAD and RCA hypohynetic, No AS/MS. Severe LV dysfunction, Sclerotix AV, Diastolic dysfunction Present.
Random blood sugar -80mg/dl
USG ABDOMEN AND PELVIS :B/L GRADE 2 RPD CHANGES,GRADE 2 FATTY LIVER, MILD ASCITIS.
TREATMENT
DAY 1
25% DEXTROSE IV /SLOW
IVF 10%D AT100ML/HR
INJ.PANTOP 40MG IV/OD
GRBS AND BP MONITORING HOURLY
DAY 2
5%DEXTROSE AT 50 ML/HR
IVF 10% D AT 100ML/HR
INJ.CEFTRIAXONE 1GM /IV/BD
INJ.PANTOP 40 MG IV/BD
TAB ATENOLOL 50MG PO/OD AT 8 AM
GRBS AND BP 4TH HOURLY MONITORING
STOP OHA TILL FURTHER ORDERS DAY 3
5%DEXTROSE AT 5O ML/HR
IVF 10% D AT 100ML/HR
INJ.CEFTRIAXONE 1GM /IV/BD
INJ.PANTOP 40 MG IV/BD
TAB ATENOLOL 50 MG PO/OD AT 8 AM
DAY 3
GRBS AND BP 4TH HOURLY MONITORING
STOP OHA TILL FURTHER ORDER DAY 4
5%DEXTROSE AT 50ML/HR
IVF 10%D AT 100 ML/HR
INJ.CEFTRIAXONE 1GM/IV/BD
INJ.PANTOP 40MG IV/OD
TAB ATENOLOL 25 MG PO/OD AT 8 AM
TAB NICARDIA
GRBS AND BP 4TH HOURLY MONITORING
STOP OHA TILL FURTHER ORDERS
Advice at discharge:
TAB PANTOP 4O MG PO/OD FOR 5 DAYS
TAB LASIX 4OMG PO/BD FOR 5 DAYS
TAB NICARDIA 10 MG PO/TID FOR 5DAYS
TAB RAMIPRIL 2.5 MG PO/OD FOR 5 DAYS
LOOK FOR HYPOGLYCEMIC SYMPTOMS
PROTEIN DIET 2 EGGS/DAY
NEPHRO LP PROTEIN POWDER PO/OD 1 SCOOP IN CUP OF MILK
FOLLOW UP
Review of after 1 week.